
BIOSAFETY TRAINING 2016











OBJECTIVE
The “Laboratory Biosafety Training
Course” aims at training laboratory professionals in
biosafety and biorisk management according to the highest
international standards, promoting the knowledge and the dissemination of these
standards in Italy and abroad, with particular attention to developing
countries.
PARTICIPANTS
The presence of about 10 (maximum) participants from all over the world
is envisaged. Although candidates will have homogeneous bio-medical
background, the variety of presented topics addresses the needs and
interests of different professionals in the field of bio-risk management.
Good command of English is required.
INFO
Please download the registration form here.
Thanks to generous sponsors, CLIMVIB is pleased to announce a public competition for two scolarships which aim at promoting the participation of scientists from low and low-middle-income countries. For more information click on the links below!
Laboratory Biorisk Management
Martien Broekhuijsen
Biorisk is defined[1] as the combination of the probability of
occurrence of harm and the severity of that harm where the source of
harm is a biological agent or toxin. Biorisk management is a management
system to manage the biorisk in an organisation. Any organisation that
contains facilities where work is carried out with potentially hazardous
biological materials or genetically modified organisms (GMO) should
implement a biorisk management structure and policy.
A successful biorisk management system relies on commitment by the top
management and a focus on continual improvement. Biorisk management
starts with a risk assessment based on planned projects with biological
agents. At the same time, the organisation must obviously follow any
applicable legislation.
Many of the elements of a biorisk management system are also implied by
general biosafety measures. However, the management system involves a
higher level system to ensure that the organisation as a whole (top
management, middle management, and all other involved employees) is
functioning in a coordinated manner. It also implies monitoring,
corrective actions, and reviewing.
An effective management system approach[2] should be built on the concept of continual
improvement through a cycle of planning, implementing, reviewing and
improving the processes and actions that an organization undertakes to
meet goals. This is known as the PDCA (Plan-Do-Check-Act)
principle.
Recently, as part of a biorisk management system, the competence of
biosafety professionals is increasingly seen as a crucial success
factor. The International Federation of Biosafety Associations[3] (IFBA) has published a
handbook “Ensuring Quality Biorisk Management Through
Certification of Professionals”.
[1] CEN
Workshop Agreement CWA 15793 (2011) “Laboratory biorisk
management”.
[2] CEN Workshop Agreement CWA
16393 (2012) ” Laboratory biorisk management - Guidelines for the
implementation”.
[3]
http://www.internationalbiosafety.org/
Laboratory Biosafety
Martien Broekhuijsen
According to a very general definition,
biosafety is the prevention of large-scale loss of biological integrity,
focusing both on ecology and human health[1]. Related fields are ecology, agriculture,
medicine, chemistry, exobiology, and synthetic biology. Several
international treaties or conventions cover one or more of these topics.
In this lecture the term biosafety will be limited to laboratory
aspects. This is relevant for any field where potentially hazardous
biological materials or genetically modified organisms (GMO) are used in
a laboratory facility.
The main focus in such a setting is on containment and protection of
workers. Containment is required to prevent escape from the laboratory
and spread into the environment of potentially hazardous biological
materials (mainly: pathogens). A pathogen can be any infectious agent
(virus, bacterium, fungus, parasite, prion), mainly human pathogens, but
also animal and plant pathogens which can have devastating effects on
agriculture, economy, or ecology. In addition, non-infectious agents can
include biological toxins, GMO’s, or as yet not clearly defined
synthetic biological entities.
The basic approach since many years has been to define four risk levels,
referred to as risk groups 1, 2, 3, and 4, with risk group 4 being the
highest risk level. For each level, specific risk control measures are
described, including physical measures (construction, barriers,
ventilation, PPE), organisational measures (roles, functions,
responsibilities, training), administration (biosafety manual,
procedures, licences, database), and monitoring measures (validation,
inspection).
Several guidelines or biosafety manuals that describe these control
measures can be found on internet, including from the WHO[2], CDC[3] (US), Canadian government[4], and the EU[5],[6]. In addition, several countries
have national legislation or guidelines. This lecture will not focus on
these specific documents, but on the general principles of biosafety and
its implementation.
Biosafety knowledge exchange is provided by several national and
international biosafety associations, such as EBSA and ABSA.
[1]
Wikipedia (https://en.wikipedia.org/wiki/Biosafety)
[2]
http://www.who.int/csr/resources/publications/biosafety/WHO_CDS_CSR_LYO_2004_11/en/
[3]
http://www.cdc.gov/biosafety/publications/bmbl5/
[4]
http://canadianbiosafetystandards.collaboration.gc.ca/
[5] EU directive 2000/54/EC on
protection of workers from risks related to exposure to biological
agents
[6] EU directive 2009/41/EC on the
contained use of genetically modified micro-organisms
Laboratory Biosecurity, Dual Use of
Biological Materials and Ethical Issues
Tatyana Novossiolova
The purpose of this two-hour lecture is to provide an overview of the following key concepts:
- Biosecurity;
- Dual Use;
- Ethical, Social, and Legal Responsibilities of Life Scientists.
The lecture looks into the core principles of
biosecurity and the role of various stakeholders in promoting and sustaining
biosecurity locally, nationally, and internationally.
The lecture further aims to foster an understanding of the concept of dual
use and how it relates to the life sciences in the 21st century in terms of
responsibilities and practices.
The lecture covers the basic elements of the new International Certification
Programme in Biosecurity that was launched by the International Federation
of Biosafety Associations (IFBA) in spring 2016.
The format of the lecture is participant-centred featuring practical tasks
and discussion-based exercises, that are designed to encourage reflection,
debate, and active engagement with the issues to be discussed.
Key Reference Reading:
Simon Whitby et al. Preventing Biological Threats: What You Can Do,
(Bradford: University of Bradford, 2016).
Tatyana Novossiolova, Biological Security Education Handbook: The Power
of Team-Based Learning, (Bradford: University of Bradford, 2016).[1]
[1] Both books are freely available at: http://www.bradford.ac.uk/social-sciences/peacestudies/research/publications-and-projects/guide-to-biological-security-issues/
Regulatory Aspects
Martien Broekhuijsen
Most developed countries have legislation
for work with biohazardous materials at a national level, including
authorities and inspection bodies. All EU member states fall under the
European biosafety legislation. The biosafety rules that apply in the US
and Canada are often considered in the EU as valuable resources for
comparison. There is extensive overlap between the various
guidelines.
There is a basic distinction between legislation for work with naturally
occurring hazardous biological agents (BA) and genetically modified
organisms (GMO). Although risk assessment, risk levels, and safety
measures are often comparable between work with either BA or GMO, there
can be very relevant distinctions. At the EU level, there are specific
guidelines for BA[1] and for GMO[2]. Specific legislation exists
for transport of hazardous biological materials, e.g. the Dangerous
Goods Regulations of IATA[3].
Additional legislation might exist for publication of knowledge, dual
use, import and export, use in environment (especially for GMO), and use
in agriculture or food.
Legislation and guidelines can change over time. This can be caused by
new knowledge of biohazard, evolving insight, or newly discovered
pathogens. The planned eradication of poliovirus is causing the WHO to
issue plans[4] for stricter safety
rules for work with poliovirus.
Accreditation is the process in which certification of competency,
authority, or credibility is presented[5]. If compliancy is concluded by an
independent third party, an official written statement (certificate) is
issued to confirm this. Certification is a more loose term that refers
to the confirmation of certain characteristics of an object, person, or
organisation[6]. Usually this is
accomplished by some form of external review or audit. Organisations
that issue certificates are often in turn accredited by official
accreditation bodies, which are established in many countries with the
primary purpose of ensuring that conformity assessment bodies are
subject to oversight by an authoritative body[7]. Certification does not state an absolute
level of competency, but establishes compliancy of something with a set
of requirements. Compliancy is not meaningful if the requirements are
not clearly described. In many cases certification is based on
internationally established standards such as ISO.
[1] EU
directive 2000/54/EC on protection of workers from risks related to
exposure to biological agents
[2] EU directive 2009/41/EC on the
contained use of genetically modified micro-organisms
[3]
http://www.iata.org/publications/dgr/Pages/index.aspx
[4]
http://www.polioeradication.org/Portals/0/Document/Resources/PostEradication/GAPIII_2014.pdf
[5]
https://en.wikipedia.org/wiki/Accreditation
[6]
https://en.wikipedia.org/wiki/Certification
[7] International Accreditation
Forum (IAF), http://www.iaf.nu
Primary Barriers: PPE & Laboratory
equipment
Martien Broekhuijsen
Personal protective equipment (PPE) consists
of a wide range of equipment and materials that are worn by a person in
order to protect him/her against biohazardous materials. Examples are
gloves, boots, coveralls, eye and face protection, and breathing
protection. The proper use of PPE is essential for biosafety. The user
must be trained sufficiently. Training with live agents is very
effective for building confidence. Training must include the correct
donning (putting on) and doffing (taking off) of PPE. Decontamination of
a person still wearing PPE is often a standard part of work before
doffing. Usually a sequence of steps is chosen to exit from the hot zone
via the decontamination area to the safe zone. Doffing of PPE in the
correct order is part of such a sequence.
There is no standard PPE, not even for a specific biosafety level. PPE
must always be adapted to the specific work conditions and surrounding,
and especially to the particular infectious organism being handled.
Knowledge of the usual routes of infection of an organism helps in
selecting the appropriate PPE components.
PPE should not inhibit the work to be carried out. PPE should also not
pose a high burden upon the worker, as this might encourage a worker to
not consistently using it. This relates to weight and general comfort,
but also to heat and moisture building up inside a coverall. Breathing
should be easy even under moderately stressful work conditions.
Biosafety equipment is any type of equipment that is used for containing
biohazardous materials inside the biosafety area, for preventing the
spread of such materials, or for protecting workers against contact with
such materials.
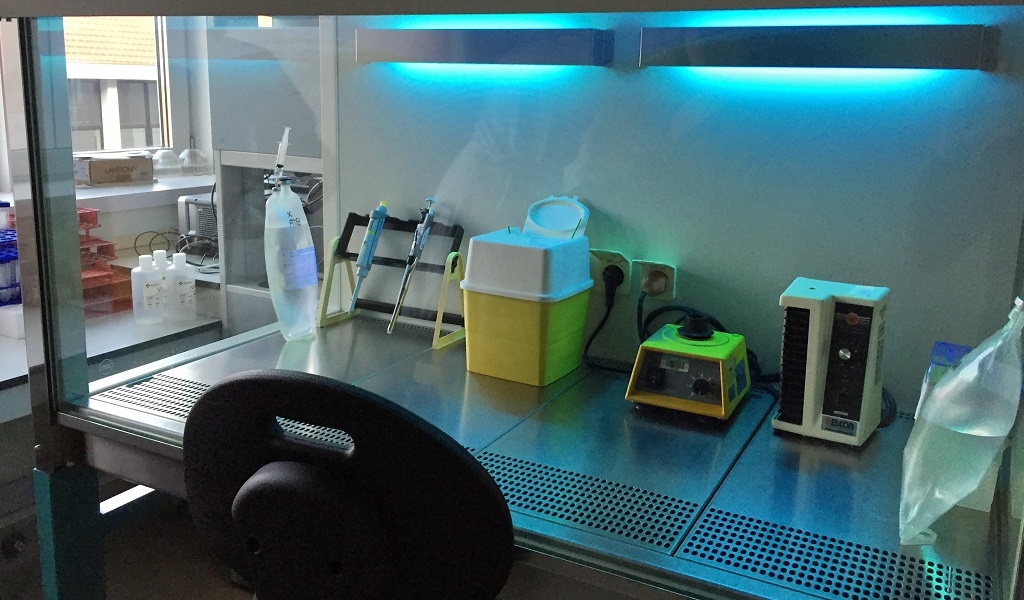
Perhaps the most central piece of equipment is the biosafety cabinet.
Besides protecting the worker and preventing spread of materials in the
laboratory (or outside), they also protect the biological materials from
becoming contaminated with biological materials from the environment or
even from within the work space inside the cabinet (cross
contamination). Several types of biosafety cabinets exist, with
different properties and adapted to different kinds of work or risk
level. The proper use of biosafety cabinets is crucial to their
performance and workers need to be trained for doing so. The placement
of biosafety cabinets in a room and connection to the ventilation system
are also important factors to address.
Secondary Barriers: Facility design and
construction
Gijsbert van Willigen
The principles of biohazard control centre
on the concept of containment. The purpose of containment is to
eliminate or reduce exposure of the environment and the outside
environment from potentially dangerously pathogens. Using containment
infectious agents can be handled in laboratory in a safe way.
There are three major elements of containment:
- Laboratory practices and techniques, i.e. Good Laboratory Practices
- Safety equipment, i.e. primary containment
- Facility design and construction i.e. secondary containment
Facility design and construction contributes
to the laboratory workers protection, provides a barrier to protect
humans and animals outside the laboratory and provides protection from
infectious agents if the primary barrier has failed or collapsed.
The strength of secondary containment depends on the risks that are
posed by the biological agent. Secondary containment of a BSL1 or BSL2
laboratory can consist of a separation of the lab from public areas,
hand washing facilities and the availability of an autoclave in the
building.
When the risk of the agent increases or the transmission route is via
aerosols multiple layers of secondary containment measures may become
necessary to prevent escape of the infectious agent from the laboratory.
These extra layers of secondary containment include the use of
specialized Heating, Ventilation and Air Conditioning systems (HVAC
systems) to ensure “negative differential pressure” or “inward
directional airflow “, treatment of exhaust air using HEPA filtration to
remove infectious agents from the exhaust air, the use of airlocks for
entrance, controlled access, building management systems and even
security systems to prevent theft of the infectious agents from the
facility.
In the presentation the concepts of secondary containment together with
the challenges from an engineering and users point of view will be
discussed. The BSL3+ facility of the Leiden University Medical Center
will be used as an example where biosafety and biosecurity are well
integrated into one facility.
Good Laboratory Practices
Martien Broekhuijsen
Good laboratory practices are all those methods
and procedures that in combination with other measures (e.g. physical
barriers or equipment) ensure the safe handling of hazardous biomaterials.
In several countries the most often used description is Good Microbiological
Practice (GMP), not to be confused with Good Manufacturing Practice. Other
terms used include Standard Microbiological Practice (SMP) or Safe
Microbiological Practice (also SMP).
Any biosafety procedure or biosafety equipment can be rendered useless if
the user makes mistakes or does not use the equipment properly. The correct
use of equipment and proper execution of methods by the microbiological
worker is at the core of biosafety. A proper level of education and
sufficient training are the most essential starting points for GMP.
Many international guidelines include paragraphs on GMP, such as from the
WHO[1], CDC[2], and others. International biosafety
associations such as ABSA and EBSA also publish guidelines for GMP.
GMP involves aspects such as training, peer control, procedures, SOP’s, and
other elements. Several organisations offer training courses for GMP. Many
use videos and photos to illustrate essential elements of GMP. GMP is not a
replacement for a microbiological education, it is merely an extension,
relying on a solid microbiological education as basis.
[1]
http://www.who.int/csr/resources/publications/biosafety/WHO_CDS_CSR_LYO_2004_11/en/
[2]
http://www.cdc.gov/biosafety/publications/bmbl5/
Biohazardous Waste
Management
Gijsbert van Willigen
Solid (including sharps) or liquid biohazardous
waste is unavoidably produced in facilities where laboratory experiments,
experiments with animals are performed during the treatment of patients. For
save handling of this waste it should be collected in such a way that it
does not pose any risk for the people who handle or transport this waste
inside or outside of the institute. Special bags, over packs and containers
should be used for safe collection of biohazardous waste. They should be
leak and puncture proof and can be used for various types of
decontamination. Preferably they cannot be reopened. For biohazardous waste
national and international legislation is in place for dealing with
biohazardous waste.
For inactivation of biohazardous waste several methods are available ranging
from chemical inactivation to various types of a physical process for
inactivation. All these methods aim at rendering the biohazardous waste
harmless for humans, animals and environment. Depending on the risk, this
inactivation should take place outside the organisation (BSL1 and BSL2) or
within the organisation (BSL3 and BSL4)
The method of choice for inactivation of biohazardous waste greatly depends
on the composition and volume of the waste, the risk level of the waste, but
also if the material that is being decontaminated is reusable or disposable.
Also economic factors can be considered when choosing an inactivation
method. After a method is chosen the inactivation process must be
validated.
For a proper inactivation, validation and verification of the inactivation
process should be in place. For this several methods can be used to
demonstrate the effectiveness of the inactivation. One of them is the use of
biological indicators when physical processes are used for
inactivation
In the presentation all aspects of biohazardous waste management will be
discussed. Also some of the commonly made mistakes will be shown.
Laboratory Accidents
Davide Mileto
The security of work place is one of the most
important aspects of the working activity. The risk assessment for the
scientific laboratory, chemical and biological, is linked with the presence
of hazardous factors present in the daily lab activities. Among the
different elements to be considered in a risk assessment, there are the
agents, the equipment, the problems linked with the space limitations,
organizational/management aspects and sometimes the lack of information,
education and training of the staff. The presence of these factors in a
laboratory setting could cause laboratory accidents, such as break of tubes
in a centrifuge, projection of liquid in eyes, spills, accidental injection
of a contaminated solution, aerosol of liquid solution that could generate
the spread of agents into the laboratory environment thereby causing the
infection of workers or the contamination of equipment and materials, etc.
Accordingly, a relevant problem in the context of the laboratory accidents
is all infection acquired through laboratory or laboratory-related
activities regardless whether they are symptomatic or asymptomatic in
nature. This infections are defined as Laboratory Acquired Infection (LAI)
or laboratory-associated infections. Among the LAI, the bloodborne Pathogens
are important especially for HBV, HCV and HIV infections.
A prevention plan is mandatory to minimize the risk of accidents. Every
laboratory should perform a risk assessment in order to evaluate which are
the risks that could be encountered inside the laboratory. Risk assessment
must take in account every material, every procedures, workers, environment
and the different protective equipment. In the context of laboratory
accidents, personnel training plays a key role: the workers are directly
exposed to risk in case of emergency and they are the first operators
involved in emergency maneuvers.
Laboratory Acquired
Infections
Romualdo Grande
Laboratory-acquired infections due to a wide variety of bacteria, viruses, fungi, and parasites have been described. Although the precise risk of infection after an exposure remains poorly defined, surveys of laboratory-acquired infections suggest that Brucella species, Shigella species, Salmonella species, Mycobacterium tuberculosis, and Neisseria meningitidis are the most common causes. Infections due to the bloodborne pathogens (hepatitis B virus, hepatitis C virus, and human immunodeficiency virus) remain the most common reported viral infections, whereas the dimorphic fungi are responsible for the greatest number of fungal infections. Because of the increasing attention on the role of the laboratory in bioterrorism preparation, I discuss the risk of laboratory-acquired infection with uncommon agents, such as Francisella tularensis and Bacillus anthracis. Physicians who care for a sick laboratory worker need to consider the likelihood of an occupationally acquired infection while advising exposed laboratory workers about postexposure prophylaxis. In addition, physicians should be aware of the importance of alerting the laboratory if infection with a high-risk agent is suspected.
Introduction to Occupational
Medicine
Angelo Moretto
The aims of occupational medicine are the
identification of health risks in the workplace, health surveillance of
workers, diagnosis and treatment of occupational diseases, and in
collaboration with professionals with other expertise (e.g. engineers,
chemists, industrial hygienists, psychologists) participation to training
programs and activities of risk management measures. Over the year, a shift
has been observed in the attitude towards health and safety in the
workplace. From the XVIII century Bernardino Ramazzini’s first textbook on
occupational diseases to the modern legislation, the active involvement of
the workers has been increased. In fact, in the XXI century workers are
required to actively participate in the management of health and safety in
the workplace. This has two consequences: on one hand workers are entitled
to provide suggestions and participate in the planning of the activities
related to their health and safety through their representatives; on the
other hand workers also became responsible and liable of their behaviour
with respect to their and their co-workers’ health and safety.
Accidents (injuries) in the workplace, and occupational or work-related
diseases are taken care of by specific insurance schemes, that may differ
between countries, even within the European Union. According to the
Organisation of Economic Co-operation and Development (OECD) “An
occupational injury is any personal injury, disease or death resulting from
an occupational accident; an occupational injury is therefore distinct from
an occupational disease, which is a disease contracted as a result of an
exposure over a period of time to risk factors arising from work activity”.
Instead, the term occupational disease “is linked to the identification of a
specific cause-effect relationship between a harmful agent and the affected
human organism. However, it is not easy – and considerably more difficult
than in the case of accidents – to prove that a disease is occupationally
conditioned, i.e. caused by conditions at, not outside work”. Because of the
difficulty in proving a disease to be occupational in origin, most countries
have produced lists of prescribed occupational diseases. These are generally
limited to those diseases where a strong cause-effect relationship has been
proven. However, with the number of categories ranging from 50 to 90,
national lists vary in terms of those diseases recognised as occupational.
Recommended lists developed by the International Labour Organisation and the
European Communities seem to have led only to limited degree of
harmonisation. In addition, in certain countries, including Italy, the list
is not prescriptive, and any worker can claim a disease as occupational or
work-related provided that she/he is able to prove the causal relationship.
Each country has different legislative approaches related to registration,
notification, and compensation for occupational injuries or diseases and
their health consequences.
The risks related to exposure to biological agents at work are subjects to
an EU directive (2000/54/EC of 18 September 2025). This Directive has
general provisions that have been implemented by local legislation in EU
member Countries. General provisions of the directive include the
definitions and the assessment of risks. Employers’ obligations including
replacement, reduction of risks, information to authority, provision of
adequate hygiene and individual protection devices, information and training
of workers, compilation of a list exposed workers, active participation of
workers, and notification to the competent authority. In addition, health
surveillance, measures for the workplace, classification of biological
agents based on their characteristics. The class of the biological agent
will determine the different provisions that should be taken to protect the
health and safety of the workers, and the consequent administrative,
technical, preventive and sanitary measures.
BSL3: Agents &
Specificities
Alessandra Lombardi, Alessandro Mancon
Microorganisms are internationally classified by
a risk group (1,2,3,4).
Different microorganisms (viruses and bacteria) are reported as high
priority agents that pose a threat to national security. They can be easily
disseminated or transmitted person-to-person, cause high mortality, with
potential for major public health impact, might cause panic and social
disruption and require special public health preparedness.
For their diagnosis different methods are used: microscopy, molecular tests,
antigens and antibodies.
BSL 3 agents pose a risk for operators and
communities. For this reason, their manipulation requires dedicated
measures, in order to minimize the occurrence of laboratory acquired
infections and the spread among the population. Different national and
international institutions (i.e.: WHO, CDC) provide indications to properly
work with these agents.
BSL 3 facilities can serve both research and diagnostic purposes; obviously,
differences related to these aims exist, mainly concerning the use of animal
models.
BSL 3 laboratories are enclosed environments: air and fluids systems are
dedicated and not shared with other areas; moreover, only authorized
personnel can enter. Such a condition can be obtained with an engineering
planning before the construction building phase. Regarding the work in the
laboratory, specific rules indicate which standards that must be followed as
regards: Personal Protective Equipment, safety cabinets, decontamination
agents, work procedures. Also emergency situations must be considered: they
need particular measures, not adopted in daily routine activity.
In the Laboratory of Clinical Microbiology, Virology and Bioemergencies
(CLIMVIB) at ASST Fatebenefratelli Sacco, a BSL 3 facility is present: its
use is strictly related to diagnostic purpose, without any animal
specificity. The examples presented refer to clinical experience and depict
a real-life situation: Biosafety rules and indications are adapted to
CLIMVIB needs and they could differ from other institutions. Naturally, each
institution must meet Biosafety principles, in order to prevent personnel
infections, epidemic and/or pandemic and related panic in the communities.
BSL4: Agents &
Specificities
Romualdo Grande, Davide Mileto
The number of Biosafety level 4 containment labs
is increasing in the world. In early 1980’s only two of such facilities were
operational in the US and now an increasing number of these are present
worldwide.
New diseases associated with high mortality and morbility have been recently
discovered, whereas others, as Ebolavirus in Africa, re-emerged abruptly in
recent times as enormous outbreaks that caused a huge number of deaths. As a
consequence of such a spreading, the workload of laboratories in the world
that are able to handle this kind of response also augmented, revealing the
necessity of improving the redistribution of resources in order to allow a
significant growth of research and diagnosis on BSL4.
This lecture will provide a short overview of the characteristics of the
viruses to be handled in BSL4 laboratories.
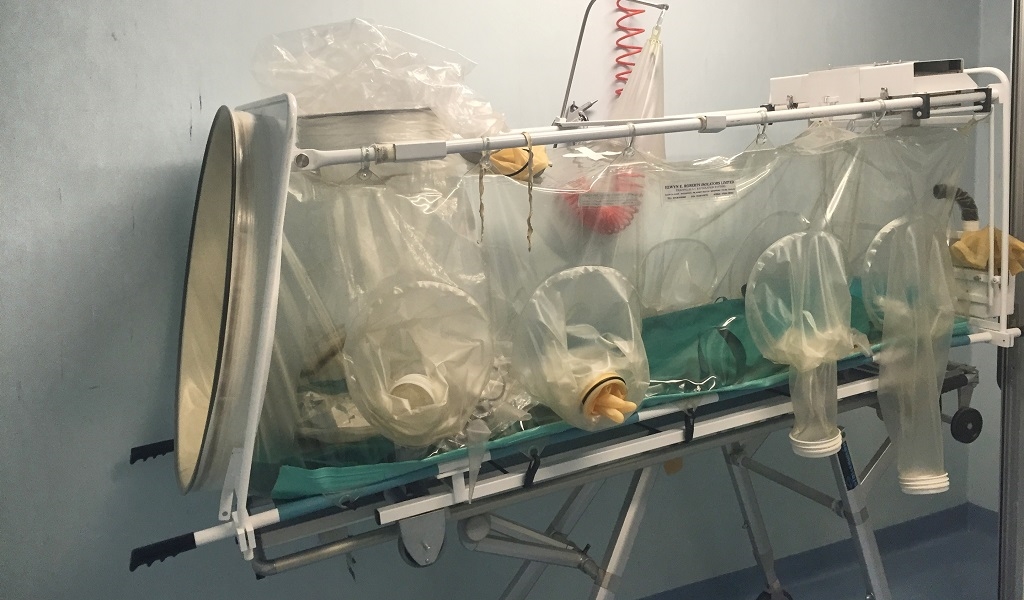
The facilities of biosafety level 4 (BSL4) are
designed in order to manage biological agents belonging to risk group 4 and
patients infected by such kind of agents.
The main feature of this facility is related with the need to avoid the
infection of workers but also with the requirement to prevent the spread of
the level 4 biological agents into the environment.
Different international guidelines (WHO or CDC guidelines) describe all the
specificities and the correct standards of behavior to be adopted for the
BSL4 facilities.
Among them surely the need to have always almost two workers inside of the
laboratory and an external support team outside of the laboratory.
Communication between the two different teams, internal and external of the
laboratory, is mandatory in order to monitor all the different steps and
procedures and to act in case of emergency. Laboratory protective clothing
must be of the type with solid-front or wrap-around gowns, scrub suits,
coveralls, head covering and, where appropriate, shoe covers or dedicated
shoes. All the personal protective equipment must be decontaminated before
being disposed of. The complexity of the structure makes it mandatory to
organize periodic training also to cope with accidents or illnesses.
Different technical features are need for the BSL4 laboratory.
A negative pressure system inside the laboratory guarantees the primary
containment. This condition is also provided thanks to the system of
interlocked door necessary to enter and exit from the laboratory. The
biosafety cabinet of level III are used inside the laboratory whereas
supplies and materials are introduced through a double-door autoclave or
fumigation chamber. A HEPA filter system cleans incoming and outgoing air
flows including the air flow need to work with the positive pressure suit.
All effluents from the suit area, decontamination chamber, decontamination
shower, or class III biological safety cabinet must be decontaminated before
final discharge.Emergency power and dedicated power supply lines must be
provided.
Via G.B. Grassi 74
20157 Milano
Railroad link
Stop Milano Certosa (4 km distant to L. Sacco University Hospital)
-Suburban line S5 (Varese – Treviglio )
-Suburban line S6 (Novara – Treviglio)
Trams
-Line 12, 19 (end of line in front of L.Sacco University Hospital)
www.atm.it
www.trenord.it
The course will take place at the Laboratory of Clinical Microbiology, Virology and Bioemergencies, of L. Sacco University Hospital, headed by Prof. Maria Rita Gismondo. The laboratory includes BSL2, BSL3 and BSL4 facilities fully equipped not only for diagnostic purposes, but also for training and hands-on educational modules.
![]()
![]()
